By Mike Koetting March 19, 2018
If it accomplished nothing else, last year’s attempt by Republicans to “repeal and replace” the ACA dramatically increased support for a single payer system. Last June, a Pew Survey found 33% of all Americans in favor of single-payer. By the end of 2017, several different polls were showing a small majority of all Americans supporting single-payer. Support among Democrats is particularly strong. A majority of House Democrats have signed on to the Medicare for All bill, as have a number of high profile senators who might be 2020 presidential candidates. There has even been discussion of making support for “Medicare for All” a litmus test for Democratic candidates.
I think there is great danger in over-investing in Medicare for All at this time.
Medicare for All has many appealing substantive features. And it is a much more appealing political slogan than a wonky let’s-fix-the-ACA. But it is very hard, I think impossible, to actually get it adopted. Among other things, it would an observable increase in taxes. Regardless of the facts, I doubt there are enough PR firms in America to convince voters that those taxes will be offset in other ways. Moreover, if this becomes serious, providers will go nothing short of bananas in their opposition. Providers have supported the ACA because it, in turn, supported their income stream. Medicare for all will be a big rate cut. Finally, there are many Americans who, deep in their soul, don’t really trust government and are scared witless at the idea of giving up their current insurance. Remember how badly it went for Obama when people, in fact, couldn’t keep their current plan. Single payer could easily become the Democrats version of “repeal and replace”—something that the base demands but is legislatively unattainable and, instead, becomes an electoral albatross. (For longer discussions, see https://thinkprogress.org/tough-questions-single-payer-7a5daec51693/ or http://onlinelibrary.wiley.com/doi/10.1111/1468-0009.12288/abstract)
So, what to do? There are in fact a handful of alternative ideas floating around for less dramatic change than Medicare for All. A few of these are described below.
- Medicare for Everyone. This is Medicare for All lite. The proposal is that everyone would automatically be enrolled in Medicare-E, a new Medicare program. Anyone who got employee-healthcare would keep their employer health and employers who did not offer comprehensive healthcare would have to contribute to Medicare. Participants not eligible for Medicaid would have payments related to their income level. Medicaid might continue as a separate program or be absorbed by Medicare-E, but state contributions would continue.
- Midlife Medicare. This is essentially Hilary Clinton’s proposal. The current ACA would continue, but a new Medicare program would be created for people over 50 (or 55) who did not have private insurance or Medicaid. There would be premiums, but the program would also be funded by general revenue, some of which would come from the same pot as the ACA subsidies for which they would otherwise have been eligible.
- Medicare X. This is a proposal by Senators Bennet and Kaine that would be offered as an option in the ACA exchanges. It would be financed by premiums and ACA subsidies, the same as other plans in the market. It would be open to anyone participating in the ACA exchange.
- Buying Into Medicaid. While not having the intuitive appeal of options involving Medicare, Medicaid actually has a set of benefits better aligned with the needs of the currently uninsured. This approach also has the advantage that it can proceed state-by-state without requiring Democratic control of everything. For instance, the leading candidate for governor in Illinois has proposed such a plan and in Nevada a similar proposal reached the governor’s desk, although he vetoed it. The fact that programs would be at the state level should lessen the argument of “federal overreach.” The program would be financed by premiums and ACA subsidies and might, or might not, be offered as an option on the ACA exchange.
Because these approaches are suggesting different things, I can’t say any of them is clearly “better”. However, some considerations follow.
- Medicare for Everyone is by far the most politically challenging. Not only will it cover a large number of people—which many will find concerning in itself—but is unlikely to attract much provider support because it would extend Medicare’s cost control mechanisms to a larger share of healthcare.
- Conversely, Midlife Medicare may be the most politically palatable because it’s the least ambitious. But it may also have difficulties attracting the further left wing of the Democrats for precisely that reason. It would contribute materially to stabilizing the ACA exchanges because it would presumably remove a relatively high cost group from the marketplace risk pool.
- Medicare X may also be relatively politically palatable, but, perversely, it might contribute to destabilization of the exchanges since its ability to draw on Medicare rates could potentially give it sufficient advantage to drive commercial plans out of the marketplace.
- Buying into Medicaid is a strategy of expediency rather than a philosophical position. It is useful to keep in mind that Medicaid is much closer in benefit structure to what many single payer advocates imagine than Medicare. The road to funding Medicaid buy-ins is not clear, but presumably possible. In fact, this approach is similar to an option already in the ACA, the Basic Health Plan. It would most likely, however, need to extend coverage beyond what is available in the Basic Health Plan option. For this to get much leverage, it would probably be necessary to improve chronically low Medicaid rates for providers.
Moving Forward
My suggestions for moving forward are less substantive and more procedural.
The most important criterion for any proposal is that it is politically feasible. I think it is important that Democrats settle on the general outline of what they are pursuing before they get too far into the debate. Otherwise they will find their intraparty differences, which are not small, will make actual passage much harder than if they narrow the discussion before-hand.
It is essential that as the proposal moves forward, it does so in open and deliberative manner; the contrast to the various Republican “repeal and replace” bills should be obvious. This is so important because at this point it seems clear that no modification of the healthcare insurance system will “stick” unless there is some real, national consensus. It is impossible to imagine a proposal that will not be adopted primarily with Democratic votes. But hopefully there can be enough cracks in the Republican façade—in public opinion if not actual votes—that it will be more difficult to make it a purely political football.
One important element of obtaining some consensus will be to avoid obvious, new, widespread tax burdens. Americans are allergic to taxes and apparently impervious to analysis of what is obtained for new taxes—or lost by the absence of taxes. Ultimately there will need to be a major reorganization of the financing of healthcare, but the more gradual and the more targeted, the more likely it will be accepted.
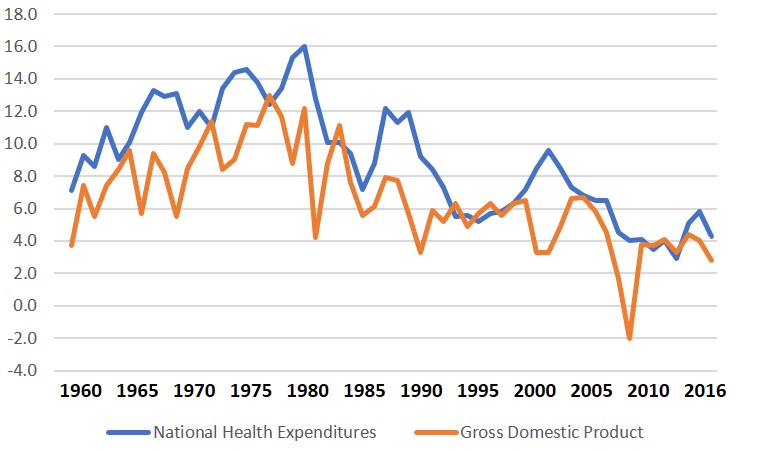
Finally, while all of the above proposals focus primarily on increasing access, the long run stability of the American healthcare system will also require controlling costs. Since 1960, year-after-year, healthcare costs have increased by roughly 40% more than GDP growth. While healthcare is not a bad expenditure, there are many other social needs. Sooner or later we are going to have to bite the cost bullet. I think every new proposal should be evaluated through that lens. Anything that proposes to reduce costs too dramatically will be difficult to pass. But gradual, concerted pressure with this clear goal in mind is necessary for the long run.
GDP vs Health Care Expenditures
Annual Percentage Increases, 1960 to 2016
A Medicare for All proposal would be a large step toward controlling costs. A worthy goal, but too large a step at this time. Trying to get it all at once is likely to leave the proposal stranded on the political beach like a woe-begotten whale. Something more gradual, which can be absorbed by the bulk of the population, is much more likely to lead to sustainable benefits.

Thoughtful. Well articulated. And a chance that it is largely true. Enjoy your time away and continue thinking deeply
LikeLike